 English
English 简体中文
简体中文
-

0.2ml PCR Octet Tubes
-

0.2ml PCR Octet Tubes - With Caps
-
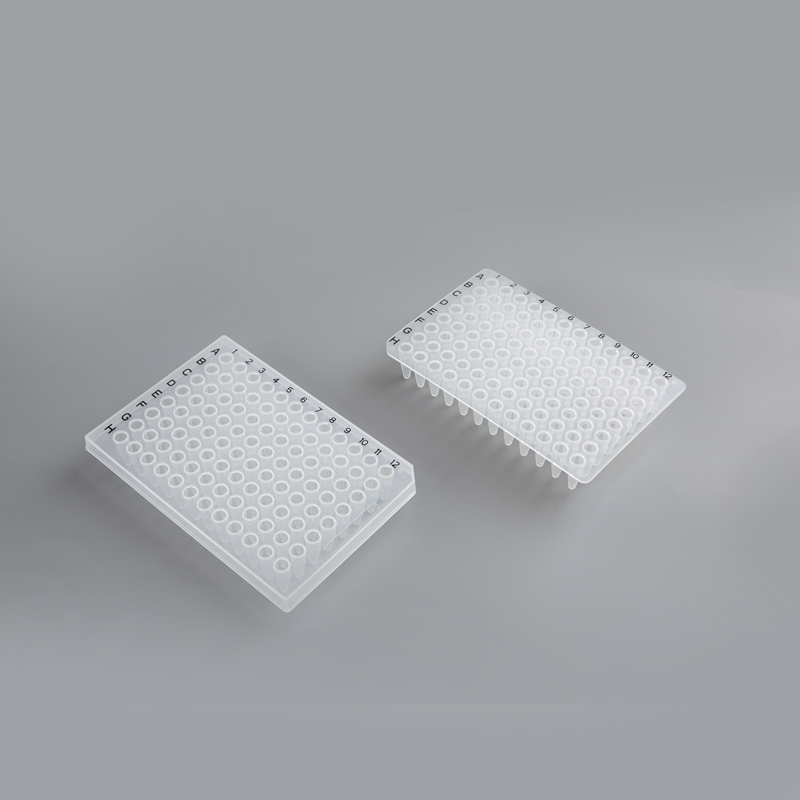
96-Well Semi-Skirted & Non-Skirted PCR Plates
-

8-Well Enzyme Strips & Plates
-
96 Magnetic Bar Sleeve
-

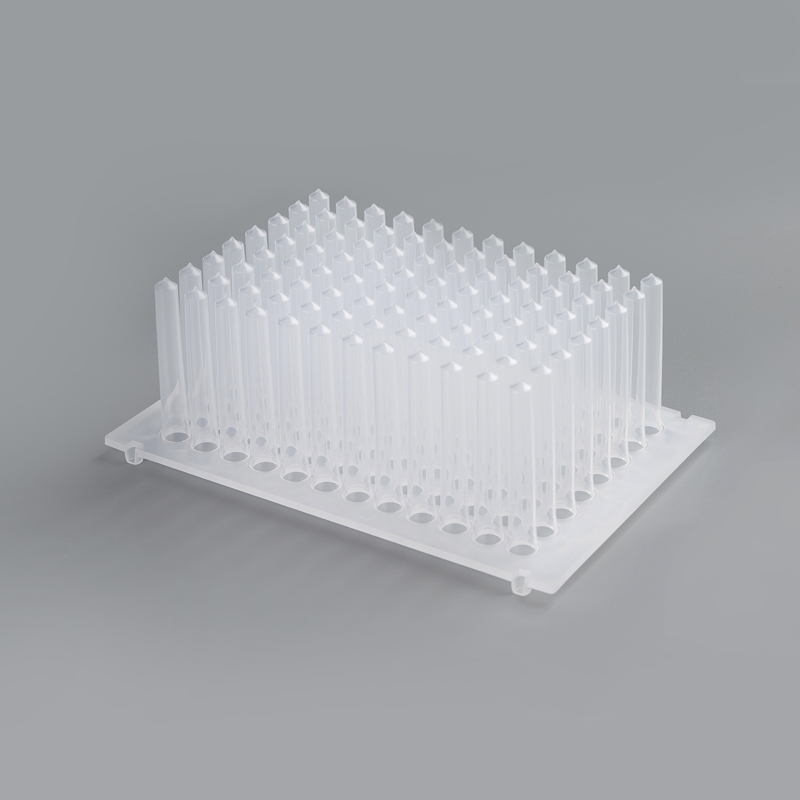
8-Link Magnetic Bar Set
-
.jpg?imageView2/2/format/jp2/q/100)
96 Round Bottom Deep Well Plates
-
-1.jpg?imageView2/2/format/jp2/q/100)
96 Cone Bottom Deep Bore Plates
-
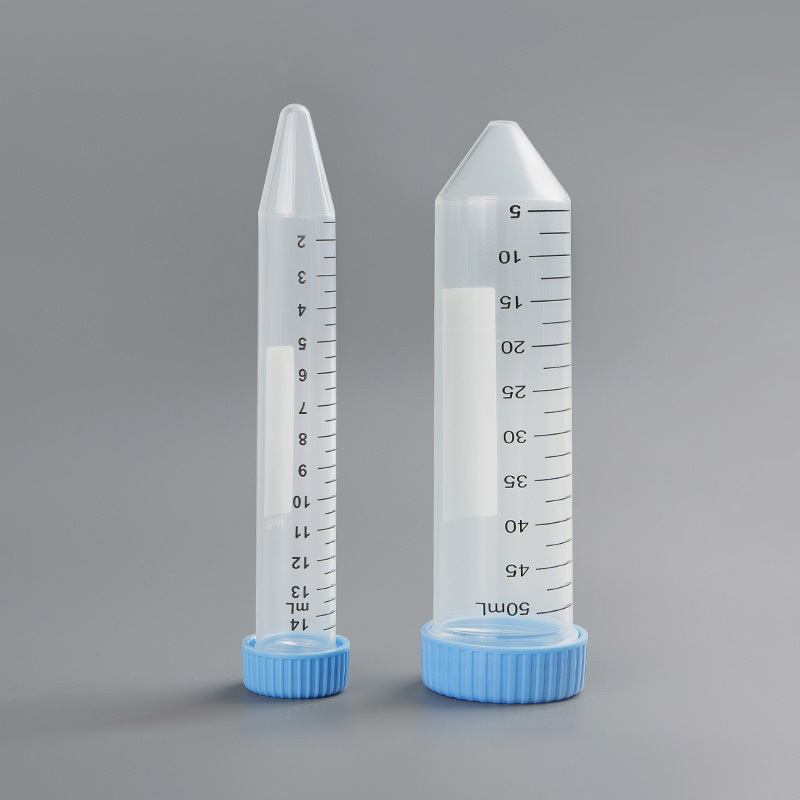
14ml 50ml Centrifuge Tubes
-

2ml 1.5ml 0.6ml Microcentrifuge Tubes


Effect of endotoxin on liver function
Posted by Admin | 13 Feb
Clinically, endotoxemia is easy to occur in severe hepatitis and decompensated cirrhosis, and endotoxin causes a further decline of liver function, forming a vicious circle. In the decompensated phase of liver cirrhosis, the ability of the liver to synthesize lipoproteins decreases, and portal hypertensive enteropathy can also occur, with intestinal mucosal barrier dysfunction, bacterial overproduction, intestinal congestion, and decreased local immune function. A combination of multiple factors can easily promote endotoxin and bacterial translocation, resulting in endotoxemia.
In blood, lipoproteins can neutralize endotoxin, especially HDL. SCD14 can promote the LPS of mCD14 binding to monocytes and macrophages to shed and transfer to HDL, which makes the activation effect of LPS disappear, but LBP has no such function. Therefore, in a way, sCD14 can negatively regulate the toxic effect of endotoxin. Plasma lipoproteins can promote the release of bacterial LPS bound on monocytes, and also reduce the activation effect of LPS. Cholic acid itself can inhibit the growth of gram-negative bacteria. Cholic acid secretion decreases when intrahepatic cholestasis occurs.
HDL mainly comes from the synthesis of the liver and small intestine. During cirrhosis, the number of hepatic parenchymal cells decreases greatly, affecting the synthesis of lipoproteins such as HDL. Intestinal congestion and nutritional disorders also affect their local immune and synthetic functions. Therefore, liver cirrhosis is prone to erogenous endotoxemia with the participation of many factors.
Related Products
CONTACT US
Leave your name and email address, we' ll get back to you soon.
 +86-512-63121818
+86-512-63121818 +86-13036212819
+86-13036212819
+86-18018109418 [email protected]
[email protected]
[email protected] No.777, Ganquan West Road, Wujiang district, Suzhou City, Jiangsu Province, China
No.777, Ganquan West Road, Wujiang district, Suzhou City, Jiangsu Province, China
