 English
English 简体中文
简体中文
-

0.2ml PCR Octet Tubes
-

0.2ml PCR Octet Tubes - With Caps
-
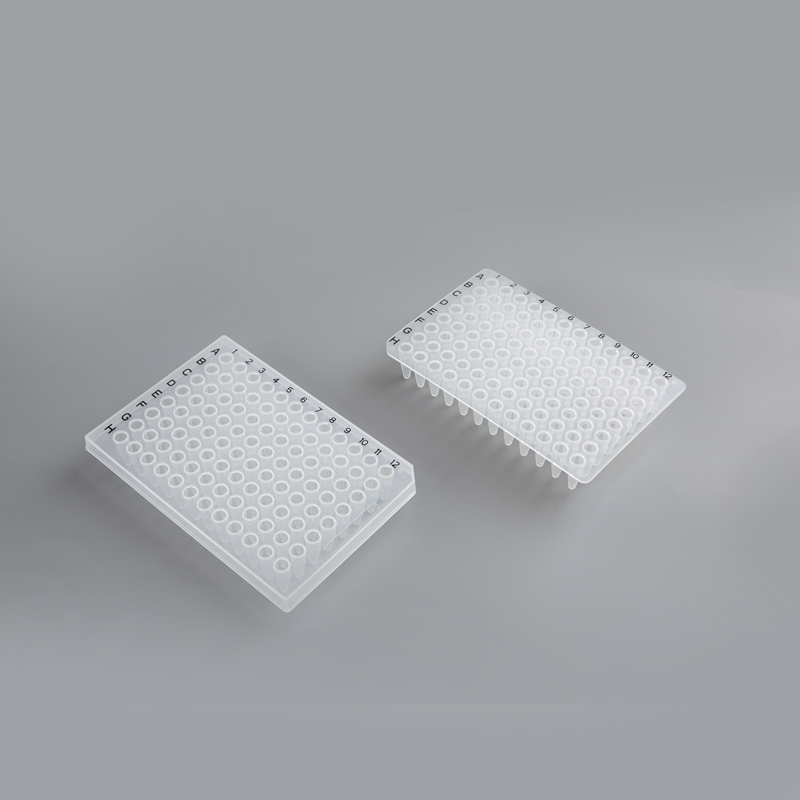
96-Well Semi-Skirted & Non-Skirted PCR Plates
-

8-Well Enzyme Strips & Plates
-
96 Magnetic Bar Sleeve
-

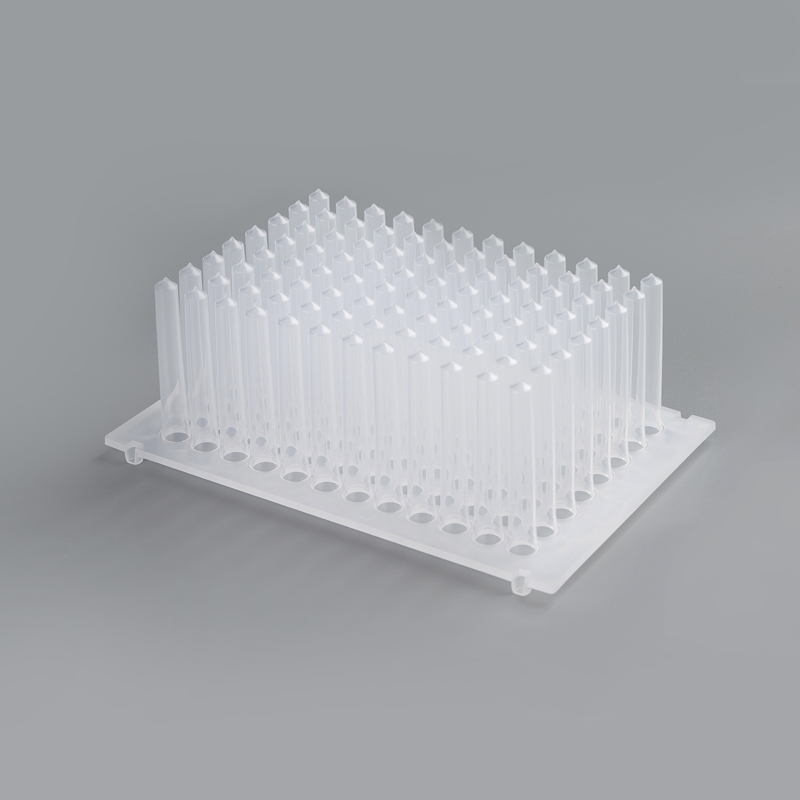
8-Link Magnetic Bar Set
-
.jpg?imageView2/2/format/jp2/q/100)
96 Round Bottom Deep Well Plates
-
-1.jpg?imageView2/2/format/jp2/q/100)
96 Cone Bottom Deep Bore Plates
-
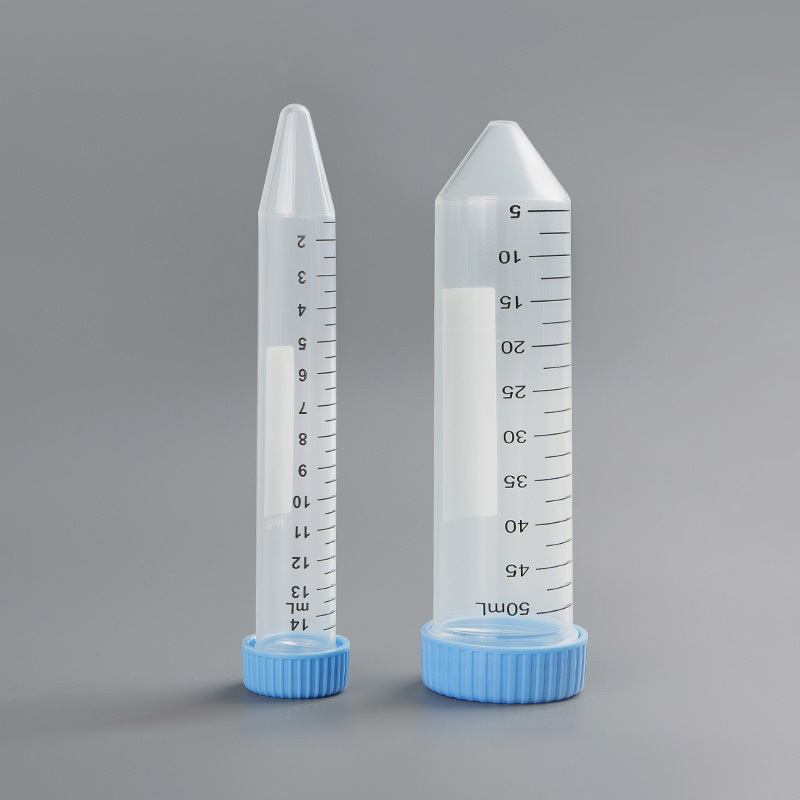
14ml 50ml Centrifuge Tubes
-

2ml 1.5ml 0.6ml Microcentrifuge Tubes


Collecting Blood in the Collecting Tube
Posted by Admin | 12 Sep
The Collecting Tube is one of several tubes used in a laboratory to collect blood for various types of laboratory tests, including biochemistry, hematology, serology and clinical microbiology. Incorrect laboratory tube collection can result in falsely increased or decreased test results which may alter patient diagnosis and treatment options. Correct tube collection is a vital step in improving the accuracy and reliability of laboratory testing.
Blood collected in the laboratory is subjected to many processes to remove any foreign material before it is drawn into the appropriate tube for a particular test or analysis. Once a specimen is placed in a tube, it is important that the tube be closed immediately. This will ensure that the sample is not contaminated with clots or other foreign materials and prevents any oxidation of the analytes in the specimen.
Once the blood reaches the inside of the tube, it is subjected to a series of chemical reactions that result in the formation of a clot on the top of the tube. This clot will then separate from the blood, making it possible to draw and analyze the resulting serum.
In the renal tubules, the shape and cross-sectional structure of each different segment differs according to its function. The proximal convoluted tubule (PCT) has a simple tall cuboidal epithelium. This epithelium is coated with a brush border composed of microvilli that increases its surface area by 30-40 fold. The cellular mechanisms that result in the transport of the major ions of the urine, such as sodium, chloride and calcium, take place in this epithelium. The distal convoluted tubule (DCT) and collecting duct (CD) are the final two segments of the kidney nephron and have important roles in both reabsorption of sodium and water. The DCT cells are also surrounded by a brush border, but the cell type that is predominant here is known as an intercalated cell, which contains both Na/K/ATPase and aquaporin, a water channel regulated by vasopressin.
When the fluid in the tubules reaches the CD, it has been reabsorbed for almost all of its sodium content. It then enters the medulla of the kidney, where it concentrates its contents to be excreted as urine. The resorption of water by the collecting duct is regulated by hormones, such as antidiuretic hormone (ADH), that stimulate or inhibit a series of protein transporters in the walls of the tubules. The late DCT and collecting duct fine tune this reabsorption by regulating the activity of these protein transporters to control sodium reabsorption, so that only a small amount of the body’s sodium is excreted in the urine. This process also conserves the body’s water stores. This concentration process is facilitated by the high concentration of sodium in the inner substance of the cells in the collecting duct wall. This is a result of the high concentration of sodium within the nephron, and the low permeability of the collecting tubule wall to water. These effects are mediated by vasopressin, cyclic 3',5'-adenosine monophosphate and the adrenoreceptors of the collecting duct.

\
Blood collected in the laboratory is subjected to many processes to remove any foreign material before it is drawn into the appropriate tube for a particular test or analysis. Once a specimen is placed in a tube, it is important that the tube be closed immediately. This will ensure that the sample is not contaminated with clots or other foreign materials and prevents any oxidation of the analytes in the specimen.
Once the blood reaches the inside of the tube, it is subjected to a series of chemical reactions that result in the formation of a clot on the top of the tube. This clot will then separate from the blood, making it possible to draw and analyze the resulting serum.
In the renal tubules, the shape and cross-sectional structure of each different segment differs according to its function. The proximal convoluted tubule (PCT) has a simple tall cuboidal epithelium. This epithelium is coated with a brush border composed of microvilli that increases its surface area by 30-40 fold. The cellular mechanisms that result in the transport of the major ions of the urine, such as sodium, chloride and calcium, take place in this epithelium. The distal convoluted tubule (DCT) and collecting duct (CD) are the final two segments of the kidney nephron and have important roles in both reabsorption of sodium and water. The DCT cells are also surrounded by a brush border, but the cell type that is predominant here is known as an intercalated cell, which contains both Na/K/ATPase and aquaporin, a water channel regulated by vasopressin.
When the fluid in the tubules reaches the CD, it has been reabsorbed for almost all of its sodium content. It then enters the medulla of the kidney, where it concentrates its contents to be excreted as urine. The resorption of water by the collecting duct is regulated by hormones, such as antidiuretic hormone (ADH), that stimulate or inhibit a series of protein transporters in the walls of the tubules. The late DCT and collecting duct fine tune this reabsorption by regulating the activity of these protein transporters to control sodium reabsorption, so that only a small amount of the body’s sodium is excreted in the urine. This process also conserves the body’s water stores. This concentration process is facilitated by the high concentration of sodium in the inner substance of the cells in the collecting duct wall. This is a result of the high concentration of sodium within the nephron, and the low permeability of the collecting tubule wall to water. These effects are mediated by vasopressin, cyclic 3',5'-adenosine monophosphate and the adrenoreceptors of the collecting duct.
Related Products
CONTACT US
Leave your name and email address, we' ll get back to you soon.
 +86-512-63121818
+86-512-63121818 +86-13036212819
+86-13036212819
+86-18018109418 [email protected]
[email protected]
[email protected] No.777, Ganquan West Road, Wujiang district, Suzhou City, Jiangsu Province, China
No.777, Ganquan West Road, Wujiang district, Suzhou City, Jiangsu Province, China
